It is impossible to escape the daily barrage of news about the CoVid Pandemic unless we were to add an additional dimension to our isolation by turning off all screens and cancelling all publications. In following the news outlets we are seeing examples of informed, decisive leadership. We are also seeing examples of responses riddled with muddled misinformation and untruths. For certain, the muddled responses are providing us with the clearest examples of the dreaded “Ds”: DENIAL (the problem does not exist); DELAY (we don’t know for certain – let’s wait and see and not disturb the economy), DODGE or DEFLECT (the questions that then come) – all leading to DEADLY OUTCOMES. Clearly, the need for evidence-based decision-making is critical with this kind of crisis.
Risk Assessment – it would be expected that progressive governance involves sound policies around societal risk assessment. Broadly speaking, risk assessment is the combined effort of identifying and analyzing potential events that may negatively impact individuals, assets and/or the environment followed by making judgments on the tolerability of such risks. Another way of putting it – prepare for the worst while hoping for the best. It is frustrating indeed to consider how different things might look had these principals been rigorously applied. Of course hindsight is 20/20 and casting back can look like a blame game. However it is a necessary exercise to acknowledge the many failings that have exacerbated this mess. That is the only way to learn for future planning.
There has been extensive research around the world and particularly in China about zoonotic corona viruses – especially the role of bats as primary carriers. The CoVid 19 virus first emerged in the Chinese city of Wuhan in December, and is thought through most investigations (but not all) to have leapt to humans at a seafood and wild-animal market (Huanan Market), where many of the first people to become infected, worked. After the SARS outbreak in 2003, the Chinese government closed wet markets and banned the ‘farming’ of wildlife. But this ban was later reversed. This is a clear failing in terms of risk management. While it is not straightforward to close these markets, the Chinese government had over 17 years to work on solutions to this, but denial and complacency set in.
The first signs of danger associated with this new (novel) corona virus were probably detected in November or early December, 2019. The Chinese government first tried to keep it quiet (and contained?) and even silenced one of the early researchers that made the information public (a Dr. Li Wenliang who later died of the disease). The Chinese first notified the World Health Organization (WHO) on December 31, 2019. This should have been done sooner. Moreover they did not initially reveal that human-to-human transfer was occurring – likely because of lack of evidence of such.
By January 23rd, 2020 Wuhan was in full lock down and the virus had spread to other countries – mostly in Asia. Despite this WHO decided that it was ‘too early’ to declare a global health emergency. This was then declared a week later but without recommending trade and travel restrictions, claiming these would be an unnecessary disruption. As well, from December 31 to January 14th, WHO and China stated that there was no clear evidence of human-human transfer. By January 23rd however, this statement was updated with the warning of clear evidence of human-to-human infection.
By March 11, WHO declared the outbreak to be a Global Pandemic. By then the CoVid virus was found in almost all countries with infections rates often doubling every 2 to 4 days. At least by then, WHO had developed a fairly reliable test, which was rapidly put to use in many afflicted countries. Those (example South Korea and Taiwan) that did extensive testing, followed by quarantine and contact tracing – along with social distancing and lock downs, demonstrated an ability to start reducing infection rates. But many of the European countries were slow to accept the gravity of the CoVid virus and infection rates ramped up drastically and rapidly.
By some measures the responses from early January through February can seem acceptable but not through the lens of rigorous risk management. The most significant failings in retrospect were the warnings about human-to-human transfer. Because of the similarity of the CoVid 19 to SARs, it would have been prudent to assume human-to-human transfer right from the onset. The primary obstacle to taking more drastic action at some of the critical points seemed to be the fear of disrupting the economy. Initial denial and delay were evident from the onset. Of course – the delays made both the health crisis and the economy much worse.
In no country was the denial/delay/dodge strategy more glaring that the USA. That is because President Trump, from mid- January until around March 10th, verbalized the denial almost daily. Six to eight precious weeks were mostly squandered. This was made worse by the unfortunate roll out of a faulty test protocol. Now the USA has the most cases worldwide and one of the highest rates of infection. These failings cannot now be re-written.
Claims by Trump and his administration that they could not possibly have been ready for this pandemic and was then misinformed by WHO, are incorrect. Seven days before Donald Trump took office, his incoming team faced a sober briefing from the outgoing Obama administration about the possibility of a global pandemic and the need to be prepared. The Obama administration had learned from the H1N1 and Ebola outbreaks. As such, the Obama administration had created a pandemic preparedness team within the White House that was then ‘reorganized’ in 2018 with the loss of expertise. Moreover, the US embassy in China initially had a large team of health professionals which was then cut over 60% by the Trump administration thereby removing expertise that would have been ‘on the ground’ at the onset of the outbreak. Furthermore – in 2018/19 a pandemic simulation conducted by the Dept. Of Health and Human Services showed the nation was unprepared for a pandemic, according to a critical draft assessment. The exercise, code named “Crimson Contagion,” had eerie similarities to the current real-life coronavirus pandemic. As well, a program funded by USAID (named PREDICT) that was set up to investigate corona viruses in bats and pangolins, was cancelled in 2019. The failings in response to this pandemic are wide spread and in many locations continuing. In most cases the failings have resulted in denial leading to delay. Delay is not an option in fighting a pandemic. It’s deadly. Time matters. Expertise matters. Evidence based decision-making matters. The countries that were much more successful in dealing with this crisis such as Germany, South Korea, Taiwan and others, prove this.
The corona virus pandemic has brought a definite urgency to the defining political question of our age: how to deal with risk on a global scale. For certain, this question also applies to climate change, which is an even greater crisis in the making. There can be no question about that. The CoVid pandemic is a crisis in fast-forward whereas climate change has been building over 50 years and counting. But the same principles of risk assessment and evidence-based decision-making, apply. Denial followed by delay of both crises is deadly.
This is a topic of great interest to me because my career was in the field of measurement science – in my case measurements for environmental contaminants. Reliable measurements are required for many aspects of our lives from ensuring safety of foods, medicines, infrastructure, water supplies and of course to the monitoring of our health. Now testing is critical for the CoVid 19 pandemic.
It has become increasingly evident that reliable, wide spread testing is one of the key strategies to slow down the rate of infection from the CoVid -19 virus. Germany is one of the best examples of this. Germany’s preparedness was helped in part by an early recognition that coronavirus was likely to become a global problem. Lacking a gene sequence for the new virus, the German team designed their first test kit based on SARS and other known coronaviruses. The protocol was published by WHO (World Health Organization) on January 17, even before the Chinese had a test. By the end of February, the Germans were producing 1.5 million test kits per week. Globally – Germany is among the lowest in infection and mortality rates.
Another of the earliest tests was developed in mainland China by the Chinese Centre for Disease Control, and details of it were posted on the World Health Organization website on January 24, just after the Wuhan lockdown was announced. Fortunately, we are seeing unprecedented speed in CoVid research thanks in large part to early Chinese efforts to sequence the genetic material of the virus that causes Covid-19. China shared that sequence in early January, allowing research groups around the world to grow the live virus. Having this viral material has resulted in research groups around the world to work on developing tests.
HOW DOES THE CURRENT TEST WORK? – A short biochemistry lesson.
The shorts version – a swab is used to collect viral material from the back of the nose, the swab is sent to a lab that isolates the genetic component. The genetic material is rapidly grown (replicated) and then detected by very specific dyes.
A more complete description – For a patient, the process of being tested for the virus is easy and can potentially be done anywhere. It is the same basic protocol used to test for other viral infections. It typically involves taking a swab from deep in a patient’s nasal cavity to collect cells from the back of the nose. The sample is then sent to a lab, where it will be tested to determine if the patient’s cells are infected with the virus.
The swabs are then tested in specialized labs that are able to look for genetic material. The genetic material in the CoVid 19 virus is called RNA – (Ribonucleic Acid). RNA and DNA (Deoxyribonucleic Acid) are nucleic acids and, along with lipids, proteins, and carbohydrates constitute the macromolecules essential for all life.
In the test – the RNA must be converted to DNA. The DNA then replicates itself millions upon millions of times until there is enough genetic material for detection. The method is referred to as “polymerase chain reaction” or PCR. The PCR test was developed by Kary Mullis from California who was awarded the Nobel Prize in 1993 for this important discovery.
The resulting genetic material during the PCR chain reaction binds with a special fluorescent dyes. During the test the fluorescence increases and the genetic material amplifies. There are variations of this test in terms of the way the chain reaction is carried out and in the manner by which the genetic material (DNA – from the RNA) is detected.
The turn around time for this standard test (as is the case for most other viral tests) usually 24 to 72 hours – mainly because of the need to transport the samples to special labs and high volume in these labs. This is clearly has not been adequate and more rapid tests are in development – see below.
WHAT HAPPENED IN THE USA?
As mentioned, China developed its own test. The WHO first adopted a test from German researchers in mid-January. These 2 protocols were basically adopted by other countries in order to produce their own tests. Some countries simply used tests provided by WHO.
The CDC (Center for Disease Control) made the decision to develop its own test towards the end of January with the intention of being the conduit for testing in the US. But there were warnings that the CDC would struggle to keep up with the volume of screening and should focus on working with private industry to develop easy-to-use, rapid diagnostic tests that can be made available to providers. Unfortunately, the CDC did the opposite. When it became clear that testing had to be ramped up, the CDC created tests kits for distribution to state labs. It soon became evident that the test kits sent were not reliable (faulty reagents). This meant that only the CDC could carry out the initial test work. As such the testing had to be restricted to only ‘high-risk patients’ who had recently travelled from China. CDC was ‘back to the drawing board and valuable weeks were lost.
This was a significant set back for the US and is one of the reasons the US has one of the highest rates of infection in the world. Fortunately, this is rapidly changing with more widespread testing now occurring.
TESTING NOW GREATLY ENHANCED AROUND THE WORLD
The short version – due to the urgency of this crisis government incentives were rapidly in place for research organizations and the private sector to develop more rapid and portable test methods. There are a number of these methods now coming on-line. It is encouraging.
A more complete version – Human ingenuity can be amazing when we face a crisis. The research efforts pertaining the CoVid virus around the world has been more than impressive. Now testing protocols have been developed in many countries with 2 main objectives in mind – 1) much more rapid and 2) being portable for use in multi-locations. For the most part – the technology is the same in that the tests focus on identifying viral genetic material. It’s the overall process that has improved in a major way. Here are just 2 examples but needless to say, there are many more.
Abbot Labs – USA – Recently (3 days ago), Abbot Labs announced a new test kit. The “ID NOW” machine as it has been dubbed can test samples one at a time. A health care provider would use a swab to take a sample from a sick patient’s nose or throat and then mix the swab into a chemical solution that breaks open the virus and releases its genetic material. The sample is then placed into the ID NOW instrument, which uses a special “isothermal technology” to replicate and amplify, if present in the sample, the small section of the virus’ genetic sequences in order to quickly detect whether a person is positive or negative for COVID-19. Such a test will allow frontline health care workers to see a patient, quickly diagnose them and make immediate decisions regarding treatment and care, thus helping prevent further transmission of the virus to other people.
Simon Fraser University – Simon Fraser University researchers will use their pioneering imaging technology — called ‘Mango’, for its bright colour — to develop coronavirus testing kits. They’re among a small set of Canadian researchers who responded to the rapid funding opportunity recently announced by the Canadian Institutes of Health Research (CIHR) to help address COVID-19. The latest research, involves using special reagents to detect individual molecules of RNA within a living cell. Dubbed the “Mango system’ it consists of an RNA Mango aptamer. Aptamers are short, single-stranded DNA or RNA molecules that can selectively bind to a specific target — in this case a special dye. The aptamer acts like a magnet – targeting and binding those dye molecules. The dye becomes excitable when bound and glows brightly. RNA molecules modified to contain the aptamer ‘magnet’ now stand out from the other parts of the cell, which makes it much easier for researchers to see and study RNA molecules under a microscope.
WHAT ABOUT A BLOOD TEST?
Short version – blood samples can be collected and tested for antibodies that are formed if a person is infected with the virus. The test mainly determines if a person had the disease rather that for use in early detection.
A more complete version – Blood tests can be very rapid and in some ways easier to get a reliable sample. To do a blood test for the CoVid 19 virus would involve analysing for antibodies to the virus. An antibody, also known as an immunoglobulin, is a large, Y-shaped protein produced mainly by plasma cells and used by the immune system to neutralize pathogens such as pathogenic bacteria and viruses.
Antibody tests are different from the typical diagnostic tests used to determine whether someone has COVID-19. As mentioned above, the latter involves taking samples of mucus and saliva and running a test in a lab to see if those samples contain the coronavirus’ genomic sequence. A serological test, on the other hand, can tell whether a person has coronavirus antibodies in 10 to 15 minutes. In some ways the test can be developed along the lines of a home pregnancy test.
To create the test, the researchers began by designing a slightly altered version of the “spike” protein on the CoVid 19 outer coat. They also isolated the short piece of the spike protein called the receptor-binding domain (RBD), which the virus uses to attach to cells it tries to invade. They then used cell lines to produce large quantities of the altered spike proteins and RBDs. Those lab-made molecules provided the basis for the test, in which antibodies in a sample of blood or plasma trigger a color change when they recognize a target protein.
This test is being used extensively in New York. But it’s main objective will be to determine who has had the disease. It will not provide early detection as it takes time for the antibodies to form in the blood stream of an infected patient.
WHAT ABOUT THE RELIABILITY OF THE TESTS
Tests are generally judged in terms of their sensitivity, accuracy (or in this case specificity) and precision (applies to quantitative tests).
The tests are proven to be “sensitive” in laboratory conditions — in this case, a technical measure of the smallest amount of the target virus they can detect. The tests must also be “specific” — for example, ensuring they do not mistake other pathogens, such as the cold coronaviruses, for the new CoVid 19 virus.
The genetic tests being used are typically very sensitive and specific under lab conditions, but in the real world, how the swab was done and the stage of illness the person was in can make a big difference. To complicate the situation, there isn’t one test. Many different tests are now being used by commercial laboratories, hospital labs and governments around the world. The interpretation of the results will therefore depend on not just the test, but other external factors.
The tests have not been around long enough to know precise information about the sensitivity and selectivity of each one. The rule of thumb that seems to becoming adopted is to assume a 5% chance of false negatives. In essence if a sick patient get’s a negative result, they should be tested again. That is acceptable given the urgency of our situation.
It is encouraging to see how quickly researchers have stepped in to enhance testing around the world. It will make a difference.
I have made some updates to my article that was initially posted on March 14, 2020. The new information is in blue font. So much has changed over the past 2 weeks. It is very difficult to keep up. In many cases – do we really want to focus on such dire news? But we must.
There is a great deal of concern and even hysteria about the spread of the corona virus. I have done a lot of research on the topic and decided to collect the information for those interested. I have a strong personal interest in this topic given that my wife is in a care home and I am currently not allowed to visit. Should we worry? Yes – to the point that we take precautions and listen to the advice coming from medical authorities. Should we panic? No – it will be temporary and the disease does seem to be peaking in China and South Korea. Moreover, the majority of those infected do not need hospitalization.
There’s no doubt though that this outbreak is upending our lives in ways that we could not have guessed even 1 month ago. There has never been a better of example of why we need evidence based decision-making. The following is the evidence taken from reputable sites such as the WHO (World Health Organization) and others.
What is a corona virus?
Coronaviruses (CoV) are a large family of viruses that cause illness ranging from the common cold to more severe diseases. The current crisis is due to a new strain that has not been previously identified in humans.
Researchers first isolated human coronaviruses in the 1960s, and for a long time they were considered generally mild. Mostly, it resulted in a cold. But the most famous coronaviruses (SARS, MERS and this one – CoVid19) are the ones that jumped from animals to humans.
NOTE – SARS – Sever Acute Respiratory Syndrome – outbreak in 2003
MERS – Middle East Respiratory Syndrome – outbreak in 2012
The name comes from the ‘studded spikes’ within the virus. It looks like a ring when viewed under an electron microscope – like a crown (corona is Latin for crown). The current corona virus outbreak – the virus was initially called novel corona virus because it is new (novel). It was more recently recently given the name CoVid 19.
Names of outbreaks matter! This is why there has been a significant outcry when a number of politicians and media personalities have been referring to this outbreak as the “Chinese Virus” of the “Wuhan Virus”. In 2015, the World Health Organization issued guidelines on how to name diseases. These guidelines stipulated that the names should NOT single out particular human populations, places, animals or food. Names that commit those sins often wind up being wrong but by then the damage can be done.
Consider for example the so-called “Spanish” Flu. That name came from a major misunderstanding. Spain was one of only a few major European countries to remain neutral during World War I. Unlike in the Allied and Central Powers nations, where wartime censors suppressed news of the flu to avoid affecting morale, the Spanish media was free to report on it in gory detail. Since nations undergoing a media blackout could only read in-depth accounts from Spanish news sources, they naturally assumed that the country was the pandemic’s ground zero. The Spanish, meanwhile, believed the virus had spread to them from France, so they took to calling it the “French Flu.” But there is also evidence that it started in the United States since the first known case was reported on March 11, 1918 – in an army base in Kansas and spread into other army bases before being transported to Europe.
It is vital that science based factors drive discussions on disease outbreaks. Global cooperation is needed as opposed to useless finger pointing. As an example – we are seeing unprecedented speed in CoVid research thanks in large part to early Chinese efforts to sequence the genetic material of the virus that causes Covid-19. China shared that sequence in early January, allowing research groups around the world to grow the live virus and study how it invades human cells and makes people sick.
Origins of COVID 19
Coronaviruses are zoonotic, meaning they are transmitted between animals and people. Detailed investigations found that SARS-CoV was transmitted from civet cats to humans and MERS-CoV from dromedary camels to humans. Several known coronaviruses are circulating in animals that have not yet infected humans.
CoVid 19 is thought to have originated in bats that in turn infected animals held for human consumption. It has also been suggested that pangolins (ant eating mammals) could be carriers.
The virus first emerged in the Chinese city of Wuhan in December, and is thought to have leapt to humans at a seafood and wild-animal market (Huanan Market), where many of the first people to become infected, worked. Pangolins were not listed on an inventory of items sold at the market — although the illegality of trading pangolins could explain this omission. These kinds of markets are referred to as wet markets and there is growing concern that they will continue to be the source of other virus outbreaks. After the SARS outbreak in 2003, the Chinese government closed wet markets and banned the ‘farming’ of wildlife. But this ban was later reversed. After the recent outbreak of the CoVid 19 – a large number of wet markets have again been closed – hopefully for good.
More information has been published of late about the role of bats. A new University of California study finds that bats’ have a fierce immune response to viral infections which likely causes the viruses to replicate more rapidly. The bats carry huge viral loads which can be easily shed and thus transfer to other animals – including humans. A research team in China is headed by a well-known virologist (Dr. Shi Zhengi) who is now known as the ‘bat lady’. Her team has identified hundreds of corona viruses – most harmless but dozens belong to the same group as SARS and CoVid 19.
‘Wet markets’ where wild and domestic animals are kept alive in cages for purchase are prevalent in warmer climates (Africa, China, SE Asia, etc) where refrigeration is scarce. There’s no doubt that wet markets were the source of SARS and CoVid 19. As such there will be an intense pressure to close these markets down. But it will not be easy as millions of poorer people rely on them for food. However, a good start would be to disallow the inclusion of wildlife in these markets. It should also be noted that factory farming of domestic animals (eg. highly crowded chicken farms in North America) could also easily become a source of viral outbreaks.
Infection route
The pathogen can travel through the air, enveloped in tiny respiratory droplets that are produced when a sick person breathes, talks, coughs or sneezes. These droplets fall to surfaces within a few feet (6 to 10 feet or 2 to 3.5 meters). That makes the virus harder to get than pathogens like measles, chickenpox and tuberculosis, which can travel 100 feet through the air. The droplets land on surfaces where the viruses can remain infections for a number of hours. When people touch these surfaces, the viruses are transferred to hands and then eventually to the face near the mouth, nose and eyes. The virus can also be inhaled from the air if close to a person who sneezes or coughs. In both cases the virus then lodges in the trachea and lungs and the infection takes hold. The incubation period is likely around 5 days. Hand washing and keeping distance from others are two of the most effective ways to prevent this route of infection.
There has been some recent reports concerning how long the virus lasts on certain surfaces. The New England Journal of Medicine just published a study that tested how long the virus can remain stable on different kinds of surfaces within a controlled laboratory setting. They found that it was still detectable on copper for up to four hours, on cardboard for up to 24 hours, and on plastic and steel for up to 72 hours. But it’s important to note that the amount of virus decreased rapidly over time on each of those surfaces and so the risk of infection from touching them would probably decrease over time as well.
Degree of contagion
Research is still in its early stages, but some estimates now suggest that the CoVid virus is 20 times more contagious than the seasonal flu. That is enough to sustain and accelerate an outbreak, if nothing is done to reduce it. Projections as to how widespread this will become vary widely. In some locations the rate of infection is increasing around 30% each day. Italy and Iran provide worst-case examples of a rapid spread. Projections for the United States vary widely with some estimates showing 1/3 to ½ of the population eventually becoming infected.
The ease by which people can become infected is the worrisome piece. In fact – 2 studies have shown that people not displaying symptoms can nonetheless spread the virus. An analysis of infections in Singapore and Tianjin in China revealed that two-thirds and three-quarters of people respectively, appear to have caught it from others who were incubating the virus but still symptom-free. It should be cautioned that these were 2 relatively small studies but it is nonetheless a note of concern.
Despite some of these more dire warnings, it is encouraging to note that when global health authorities methodically tracked and isolated people infected with SARS in 2003, they were able to bring the average number each sick person infected down to 0.4, enough to stop the outbreak. Also note – frequent hand washing can reduce the chances of infection by 50% or more.
The current growth of CoVid 19 infections is in most countries is considered to be exponential. Something is said to increase or decrease exponentially if its rate of change must be expressed using exponents. A graph of such a rate would appear not as a straight line, but as a curve that continually becomes steeper or shallower. Perhaps a better way to consider the growth is the number of days it takes for the infections to double. According to “Our World in Data” – associated with a number of prestigious universities, the rates of infections doubling are: World (number of infections doubled in 6 days), Italy (7 days), Spain (4 days), USA (3 days), Canada (4 days), China (45 days). It is clear that China’s rate of infections are levelling while most other locations are still in the exponential growth phase.
Symptoms
The coronavirus outbreak hit amid flu season in the northern hemisphere and even doctors can struggle to distinguish between the two The overlap in symptoms probably contributed to slow detection of community infections in some countries, including Italy. Typical flu symptoms, which normally come on quickly, include a high fever, sore throat, muscle aches, headaches, shivers, runny or stuffy nose, fatigue and, more occasionally, vomiting and diarrhea.
Doctors are still working to understand the full scope of symptoms and severity for Covid-19, but early studies of patients taken to hospital found nearly all of them developed a fever and dry cough, and many had fatigue and muscle aches. Pneumonia (lung infection) is common in coronavirus patients, even outside the most severe cases, and this can lead to breathing difficulties. A runny nose and sore throat are far less common, reported by just 5% of patients. The only real confirmation of having Covid-19 is taking a test though.
Mortality Rate
Early research indicates the virus may be significantly more deadly than the seasonal flu, which kills roughly one in 1,000 people. An analysis of outcomes for more than 44,000 confirmed patients in China found that roughly one in 50 died (2% mortality rate). Eighty-one percent of patients infected with the new coronavirus had mild illness, 14 percent had severe illness and 5 percent had critical illness, according to the study.
The current (as of March 12, 2020) number of cases worldwide is about 135,000 resulting in 5000 deaths. That equates to a 3.7% mortality rate. In Italy there are just over 15,000 cases with 1000 deaths (6.6 % mortality rate). In the USA – 1600 cases with 41 deaths (4.1 % fatality rate). Note – the numbers are changing daily. NOTE – see new number below.
It is assumed, however that there are many more mild cases that do not get to hospital and are not being counted, which would bring the mortality rate significantly down. Most researchers feel the true mortality will calculate to about 1 to 2 % making the CoVid 19 ten to 20 times more fatal than the flu. The mortality rate for the H1N1 (swine flu) of 2009 was 0.02%.
Deaths are highest in the elderly, with very low rates among younger people, although medical staff who treat patients and get exposed to a lot of virus are thought to be more at risk. But even among the over-80s, 90% will recover.
Some current numbers as of March 29, 2020 – 17:29 GMT
World 707,738 cases 33,526 deaths (4.74% mortality rate)
Italy 97,689 10,779 (11%)
Germany 60,659 482 (0.79%)
USA 133,146 2363 (1.7%)
Canada 6213 63 (1.0%)
China 81,439 3300 (4.0%)
One of the most notable points is the difference in mortality rate between Italy and Germany but there are considerations as to why. Firstly, Italy has one of the highest ratios of elderly residents. Secondly, it cannot be fully confirmed that each recorded death over the past month or so is directly due to the corona virus. In one study that involved a re-evaluation by the National Institute of Health, demonstrated that only 12 per cent of death certificates showed a direct causality from coronavirus, while 88 per cent of patients who died had other factors that could have contributed. A third factor is a suggested higher rate of lung issues due to air pollution and a high percentage of smoking within the population.
Is it seasonal?
Regular flu outbreaks are generally seasonal in the Northern Hemisphere. People are outside more and a degree of immunity can set in. For the CoVid 19 however, no one can say if this will be the case.
Cures and Vaccines
Efforts to develop an effective vaccine for Covid-19 have been quick compared with historical epidemics, such as Ebola. A number of teams are already testing vaccine candidates in animals and preparing to carry out small trials in people. However, the second and third phases of development will involve thousands of volunteers and will look more closely at efficacy. It is currently felt that a vaccine to protect people from the coronavirus would require a timeframe of a year or 18 months.
There is also work being done on antiviral drugs. The most hopeful at present are Kaletra, which is a combination of two anti-HIV drugs, and remdesivir, which was tried but failed in Ebola patients in west Africa in 2013 and 2016. Some Chinese doctors are also trying chloroquine, an antimalarial drug, which is off patent, therefore cheap and highly available, and would be very useful in low-income countries. The first results are expected in mid-March and should indicate if the drugs will at least help those who are most severely ill. A miracle cure is not expected.
Vaccination development is being undertaken on many fronts as is drug therapies. See upcoming article on my blog.
Going Forward
It is very difficult to predict what will happen over the coming months and year. We need to be concerned but also act in a rational way. The medical community is extremely knowledgeable with monumental efforts underway to decrease the risks we face. Life must to go on. It is crucial though that science based decisions are made.
The 3 largest impact measures will be –
TESTING – South Korea is demonstrating that testing on a massive scale is very effective. That country is testing people at a rate of 10,000 people per day. The USA is very far behind having only tested 11,000 people to date. This is a worry. Fortunately, in Canada – testing is about where it should be. It is becoming more and more clear that testing is absolutely critical in fighting this pandemic. In Canada we have so far carried out 66,000 tests (as of March 20th). This is not enough. The main reason is a shortage of supplies and a back-log in labs. In the US – the situation is more dire as the country lost about 6 weeks due to a deficient test protocol and a slow federal undertaking. As of March 20th – the US had conducted 313 tests per million people as opposed to over 6000 tests per million people in South Korea. This is changing as some new test protocols are being developed. I will write about testing in a new blog.
READYING HOSPITALS – Most hospitals are already at maximum capacity so it is important that emergency measures are considered to expand available beds and ventilators.
FULL SOCIETAL COOPERATION – it is critical that all citizens follow the advice of the medical experts – hand washing, social distancing, staying home if sick, restricting travel, avoiding large groups and getting tested if needed.
I could political here but I might get carried away. In closing – we need to pay attention to health experts — NOT politicians and nonsense flying around on social media.
The scientific consensus that the burning of fossil fuels is the main cause of global warming over the past many decade is likely close to 100 percent now. Remaining doubts seem to be mostly cleared. Despite this far-reaching consensus there is a definite disconnect of acceptance by many within the general public thereby hindering the needed and long overdue action to combat and prepare for climate change. There are a few reasons this disconnect still exists despite the mountains of evidence that continues to accumulate.
Firstly – the climate change denial groups are highly organized, well funded and well versed at undermining the evidence of global warning and the resulting changes to the world’s climate. Secondly, it is an extremely complex topic. It is very difficult to fathom that a colorless, odorless gas that we have been discharging for centuries could be the cause of a global crisis. Our brains are simply not wired to readily make this kind of connection. There can be the sense that the dire predictions could not possibly be true. Thirdly, even when we accept the need to confront climate change, there can be a reluctance to face what must be done. It will require some changes that can be perceived by some as a set-back to our way of life.
So – how do scientists – the vast majority of whom see climate change as an existential threat, communicate to general public – and thereby the elected officials that business as usual is not an option? It is easy enough to ‘preach to the converted’ and denigrate climate change deniers but that will not be enough. The goal must be to bring the vast majority of voters on board to vote for politicians prepared to take on this immense challenge. Three ideas are presented:
1. Promote the Consensus – Public opinion scholars are recommending that the broad consensus among scientists about human-caused global warming, be widely promoted. A study from Yale University labeled this as a “Gateway Belief” – that indeed the general public will be more accepting of the science of global warming and resulting climate change when the consensus message is heard repeatedly. “Perceived scientific consensus acts as a key gateway belief” wrote the authors of this study. “Repeated exposure to simple messages that correctly state the actual consensus (….). is a strategy likely to help counter the concerted efforts to misinform the public.” 2
2. Deny the deniers – For the fossil fuel industry, climate change denial is a multi-million dollar endeavour. In her book “Merchants of Doubt”, Naomi Oreskes coined the term “The Tobacco Strategy”, referencing the strategy employed by the tobacco industry aimed at stopping or at least delaying any regulation on sales or consumption of cigarettes. The “Tobacco Strategy” is for “maintaining the controversy” and “keeping the debate alive”. It doesn’t matter if there really is an argument going on or not. All that matters is for people to have that impression. This is exactly the case for the denial the science underpinning climate change.
It is extremely challenging to counter such well-funded misinformation campaigns. Their communications have a tone of credibility and for politicians that lack the courage to tackle environmental issues, these denial reports are their salvation. The first line of challenge should be to communicate that the denial reports are prime examples of bad science. The authors of the denial reports are ‘experts for hire’ and they are hired by think tanks funded by industry – most notably the fossil fuel industry. The articles they write are not published in scientific journals that require peer-review. Moreover, many (or even most) of these ‘experts for hire’ have never worked in the field of climate science.
The second line of defense is to counter each of the denial arguments pointing out how wrong they are. This must be done for each phony argument they put forward. It’s a challenge because counter-arguments can be overly complex and detailed thus possibly confusing the average reader. Nonetheless it must be undertaken using all available communication tools.
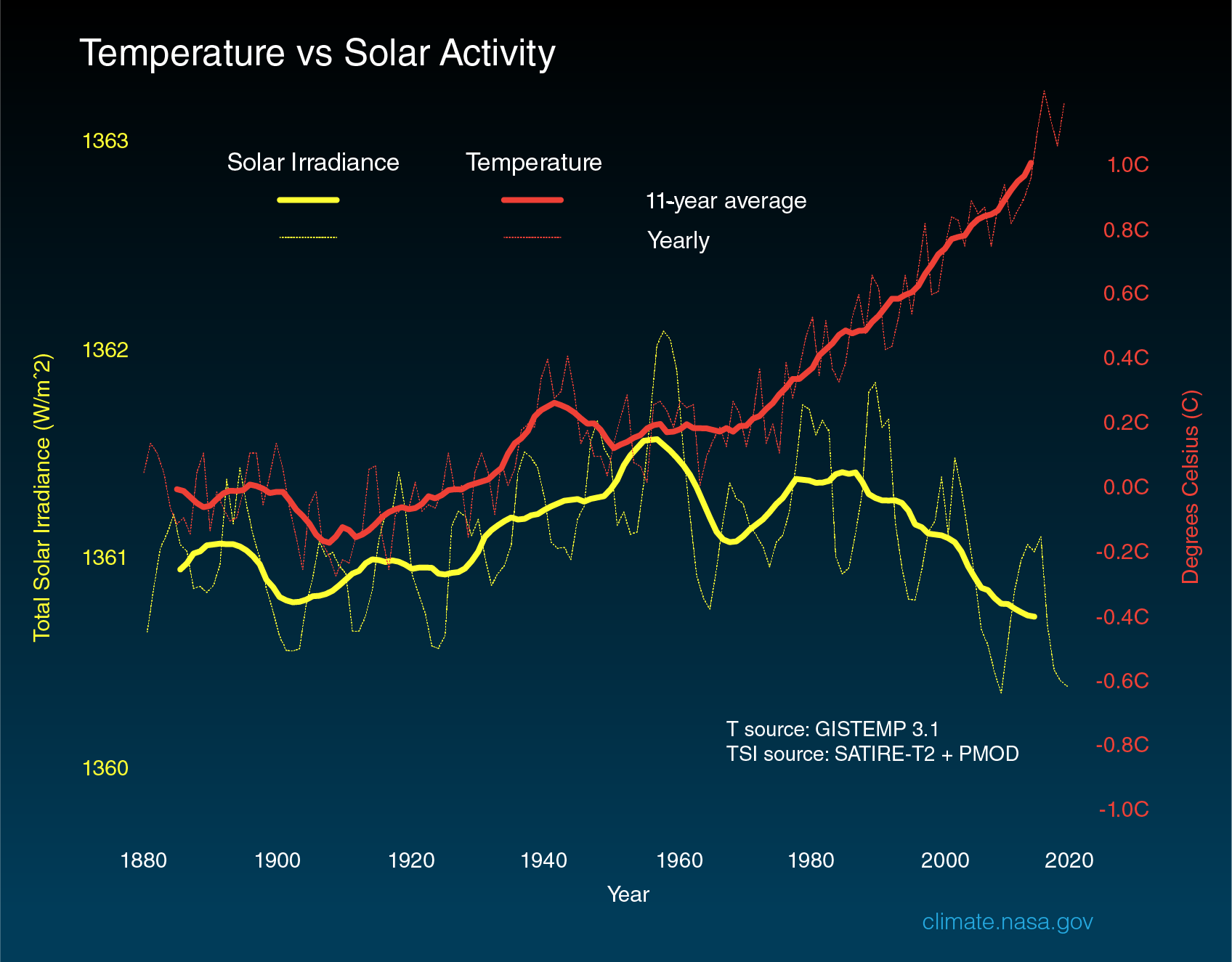
When possible, the use of graphics can greatly aid the argument. For example, one of the denial arguments is that the current warming is due to enhanced solar activity and not carbon emissions. This is simply not true. For the past number of decades solar activity has decreased.
3. Frame the Message – Communicating inconvenient science also requires a sensitivity to the values and beliefs of the audience. People do not want to be lectured or presented with an endless stream of facts and figures. It must be acknowledged that there is a reluctance, or in some cases, even an extreme resistance to hear the message. As such, emphasis away from the negative aspects (possible job losses in some industries for instance) and towards the positive is vital. Indeed, studies show that, in tackling climate change, co-benefits such as reducing deaths from air pollution and boosting technological innovation may lower the net costs of climate action to zero or even lead to a net economic benefit rather than a cost. This needs to be continually stressed.
As well, the many success stories in environmental initiatives (such as the fight to save the ozone layer) need to be told and re-told. In looking back at many of the issues now being resolved, it is clear that the truth does and will win out in the end. It takes time and the need to develop effective strategies to communicate inconvenient science.
At this critical point in humankind’s history, we must not delude ourselves. Carbon emissions from the burning of fossil fuels are warming the planet at an alarming rate. The warming of the planet is in turn affecting our climate in ways that are even more dramatic than past predictions.
THE FACTS – There is a mountain of evidence provided by climate scientists around the world that leads to irrevocable conclusion that climate change is THE issue of our times. This conclusion has been endorsed by the national science academies of almost every country in the world. It has been clear for some time now, that without monumental action on a global scale, our world is facing drastic consequences. The mean global temperature has warmed about 1 degree C since 1900 most of which has occurred since 1960. Some parts of the Arctic have warmed by over 7 degrees C. The previous decade was the warmest since records were kept.
Record-breaking heat waves are now 5 times as likely as they once were. Sea levels have risen 20 cm (8 inches) since 1900 and are now rising at an accelerated rate. As well, due to the increased carbon dioxide in the atmosphere, our oceans are becoming more acidic thus threatening sea life and coral reefs. We have seen devastating floods and landslides in some areas and extreme droughts along with related wildfires in others. These extreme weather events have been costly. The insurance industry has certainly taken note as annual climate event costs have risen from 50 billion annually in the 1980s to over 200 billion dollars annually in the last decade.
It is acknowledged that planet earth has been warm (or even warmer) in eons past. But those climate events occurring, over thousands of years, have their own explanations. The warming over the past 70 years can only be linked to carbon dioxide emissions.
MEASUREMENTS – So, how can scientists definitively claim that carbon emissions are the main causative factor? Firstly it can be stated emphatically that carbon dioxide, emitted when we burn fossil fuels, is a greenhouse gas. That is never questioned. There are other greenhouse gases in our atmosphere but none have the same radiative impact as carbon dioxide. This is what happens. Energy from the sun enters the atmosphere as visible and ultra-violet radiation that is low in heat. The earth’s surface re-emits this energy as infra-red radiation (or heat). Greenhouse gases (and especially carbon dioxide) ‘capture’ this heat, thereby warming our atmosphere. Without greenhouse gases our planet would be more than 30 degrees C cooler. The planet would be uninhabitable.
There are many ways science can make the connection between increased carbon emissions and planet warming. Carbon dioxide concentration in our atmosphere has increased from 270 parts per million (ppm) in 1940 to over 400 ppm today. When this increase is graphed with the rising temperature the correlation is remarkable.
Other climate forcings – such as volcanic and solar activity do not show this kind of correlation.
The influence of carbon emissions can also be found in the spectrum (actual wavelengths) of greenhouse radiation. Using high-resolution instrumentation, climate scientists have measured the influence of CO2 on both incoming solar energy and outgoing long-wave (heat) radiation. According to NASA, two-thirds or the warming of the atmosphere has occurred since 1975. Satellites have recorded the spectrum of the outgoing radiation over the period 1970 to 1997. Over that period, when atmospheric temperatures increased dramatically, there is a corresponding decrease in infra-red (heat) radiation. In other words – less long-wave (heat) radiation is escaping to space at the specific wavelengths of greenhouse gases. And, this corresponds to increased long-wave radiation measured at the surface of the Earth at these same wavelengths. This is empirical evidence.
UNFORTUNATE DENIAL – Unfortunately there has been a well-organized denial industry that has been successful in undermining the scientific evidence of global warming and the resulting climate change. The ‘denial industry’ refers to public relations companies that publish supposedly scientific papers that are not peer reviewed and indeed contain cherry-picked data to support a pre-ordained conclusion. These are the same kinds of companies along with their so-called ‘scientists’ that were hired to deny the truth about studies that linked lung cancer to cigarettes, industrial discharge to acid rain and CFCs (chloro-fluoro carbons) to ozone depletion. In these 3 cases they have been soundly proven wrong and they are in the process of being proven wrong about climate change. They fight science with junk-science but their message sticks. For politicians who lack the courage to confront the global warming threat (and this is especially the case now in the United State), these denial reports are their salvation.
MOVING ON – Fortunately, there is increasing hope that the existential threat of climate change is being addressed. Now that we have the Paris Agreement – a strong message has been sent to private markets regarding the need to divest away from fossil fuels and expand into low-carbon technologies. This transformation is already creating jobs and will create wealth on a monumental scale. A number of economic studies have determined that investments in energy-efficient and renewable energy sources yield more jobs for a set amount of spending than investing in maintaining or expanding the fossil fuel industry. In fact, 2014 was the first year that total world investments in renewable energy sources surpassed investments in fossil fuels and related industries. However, with the Trump administration taking the appalling step of withdrawing from the Paris agreement, there is deep worry that this impressive progress is in jeopardy.
The key elements of the Paris Accord are:
To keep global temperatures “well below” 2.0C (3.6F) above pre-industrial times and “endeavour to limit” them even more, to 1.5C
To limit the amount of greenhouse gases emitted by human activity to the same levels that trees, soil and oceans can absorb naturally, beginning at some point between 2050 and 2100 (in other words our world will become carbon neutral).
To review each country’s contribution to cutting emissions every five years so they scale up to the challenge
For rich countries to help poorer nations by providing “climate finance” to adapt to climate change and switch to renewable energy.
This will not be easy and will require a 180- degree paradigm shift in our thinking. But for the sake of our grandchildren and generals beyond, this must happen.